

























Coxarthrosis of the hip joint (HJ) is a degenerative-dystrophic disease that affects cartilage and bone tissue. In medical articles, it can be called differently: deforming coxarthrosis, DOA of the hip joint, osteoarthritis. All these terms mean the same pathology - arthrosis, but "coxarthrosis" is a narrower term that characterizes the defeat of the hip joint.
From arthrosis, the cartilage suffers first, then the bones and surrounding structures - ligaments and muscles - are involved in the pathological process. If there are changes in the bones, the word "osteoarthritis" is prefixed with "osteo". In advanced cases, there is a deformation of the joint, and we are already talking about deforming arthrosis (osteoarthritis).
general characteristics
Deforming osteoarthritis of the hip joint is the second most common after knee gonarthrosis. Due to the deep location of the hip joint, the bone deformity can go unnoticed for a long time, and the changes will only be shown on X-rays taken in later stages.
The development of this disease is influenced by various factors, including an inactive lifestyle, trauma and metabolic disorders. Precisely because of the specifics of modern life, in which there is often no place for physical education, arthrosis affects an increasing number of people. Moreover, the peak incidence falls on the middle age group - from 40 to 60 years.
Reference:coxarthrosis often affects women rather than men.
Development mechanism
The thigh joint consists of two bones: the femur and the iliac (pelvic). The head of the femur enters the acetabulum of the pelvis, which remains motionless during movement - walking, running. At the same time, the articular surface of the femur can move in several directions, providing flexion, extension, abduction, adduction, and rotation (rotation) of the thigh.
During physical activity, the femur moves freely in the acetabulum due to the cartilaginous tissue that covers the joint surfaces. Hyaline cartilage is characterized by strength, firmness and elasticity; acts as a shock absorber and participates in the distribution of loads during human movements.
Inside the joint is synovial fluid - synovium - which is necessary for lubrication and nourishment of cartilage. The entire joint is enclosed in a thick, thin capsule surrounded by strong muscles in the thighs and buttocks. These muscles, which also act as shock absorbers, serve to prevent hip joint injuries.
The development of coxarthrosis begins with changes in the joint fluid, which becomes more viscous and dense. Due to the lack of moisture, the cartilage does not get enough food and begins to dry out, loses its smoothness, and cracks appear on it.
The bones can no longer move freely as before, and rub against each other, causing microdamage to the cartilage. The pressure between the bones increases, the cartilage layer becomes thinner. Under the influence of increasing pressure, the bones gradually deform, local metabolic processes are disrupted. In the later stages, there is a pronounced atrophy of the leg muscles.
Causes
Deforming osteoarthritis of the hip joint can be primary or secondary. It is not always possible to determine the cause of primary osteoarthritis. Secondary arthrosis occurs on the background of existing diseases, as follows:
- congenital hip dislocation or hip dysplasia;
- Perthes' disease (aseptic necrosis of the femoral head);
- coxarthritis of the hip joint, which has an infectious, rheumatic or other origin;
- pelvic bone injuries - sprains, fractures.
Hip dysplasia is a congenital malformation that sometimes does not manifest clinically for a long time and in the future (at the age of 25-55 years) can lead to the development of dysplastic coxarthrosis.
Cox arthrosis can be left-sided, right-sided, and symmetrical. In primary arthrosis, concomitant diseases of the musculoskeletal system are often observed - especially osteochondrosis and gonarthrosis.
There are also risk factors that contribute to the development of the disease:
- excessive weight and excessive loads that overload the joints;
- violation of blood circulation and metabolism;
- hormonal changes;
- curvature of the spine, flat feet;
- old age;
- hypodynamics;
- heredity.
It should be noted that coxarthrosis itself is not hereditary. However, certain characteristics of the metabolism or connective tissue structure may create the preconditions for the development of osteoarthritis in a child in the future.
Symptoms of coxarthrosis
The leading symptom of osteoarthritis of the hip joint is pain in the area of the hip and groin, of varying intensity. Stiffness and stiffness during movement, decrease in muscle volume, shortening of the affected limb, and changes in gait due to limping are also observed.
Coxarthrosis usually progresses slowly, causing discomfort at first and mild pain after exertion. However, over time, the pain increases and appears at rest.
A typical manifestation of the pathology is difficulty in abducting the hip, when a person cannot sit "riding" on a chair. The presence and severity of signs of coxarthrosis depend on its degree, but the pain syndrome is always present.
There are three degrees or types of osteoarthritis of the hip joint, which differ in the severity of the injury and the accompanying symptoms:
- 1 degree. The thigh does not hurt constantly, but periodically, mostly after walking or standing for a long time. The pain syndrome is localized in the joint area, but can sometimes spread to the leg to the knee. Muscles with grade 1 coxarthrosis do not decrease in size, gait does not change, motor ability is fully retained;
- 2nd degree. Painful feelings intensify, occurring not only after running or walking, but also at rest. The pain is more often concentrated in the thigh area, but it can spread to the knees. In moments of heavy load, it is painful to stand on the injured limb, so the patient begins to spare the leg and temples. The range of motion in the joint is reduced, it is especially difficult to move the leg to the side or rotate the hip;
- 3 degrees. The pain becomes permanent and does not subside even at night. Gait is noticeably impaired, independent movement is significantly complicated, and the patient relies on a cane. The range of motion is severely limited, the muscles of the buttocks and the whole leg, including the lower leg, atrophy.
- Due to muscle weakness, the pelvis leans forward, the diseased leg shortens. To compensate for the difference in limb length, the patient leans the body to the affected side when walking. This leads to a shift in the center of gravity and increased stress on the affected joint.
Osteoarthritis or Osteoarthritis?
Arthritis is an inflammation of the joint, which can be an independent disease or develop in the background of systemic pathologies (for example, rheumatism). In addition to the inflammatory response, the symptoms of osteoarthritis (especially in the advanced stages) include limited mobility and changes in the shape of the joint.
At the heart of degenerative-dystrophic changes in arthrosis is the defeat of cartilage tissue, which often leads to inflammation. That is why arthrosis is sometimes called arthrosis-arthritis. And since osteoarthritis is almost always associated with joint deformity, the term "osteoarthritis" is applicable to it.
Reference:according to the International Classification of Diseases (ICD-10), osteoarthritis and osteoarthritis are variants of the same pathology.
Diagnosis of coxarthrosis
The diagnosis of "hip coxarthrosis" is made based on the examination, the patient's complaints and the results of the examination. The most informative method is an X-ray: in the pictures you can see both the degree of damage to the joint and the cause of the disease.
For example, in hip dysplasia, the acetabulum is flatter and curved, and the cervical-diaphyseal angle (slope of the femoral neck in the vertical plane) is greater than normal. Perthes' disease is characterized by deformity of the part of the femur located near the joint.
Grade 3 coxarthrosis is characterized by narrowing of the joint space, enlargement of the femoral head and multiple bone growths (osteophytes).
If the patient had a fracture or dislocation, signs of trauma will also be visible on X-rays. If a detailed assessment of the condition of the bones and soft tissues is needed, magnetic resonance imaging or computed tomography may be prescribed.
Differential diagnosis is made with the following diseases:
- gonarthrosis;
- osteochondrosis and radicular syndrome arising on its background;
- trochanteritis (inflammation of the trochanteric bone of the thigh);
- ankylosing spondylitis;
- reactive arthritis.
The decrease in muscle volume that accompanies grade 2 and 3 coxarthrosis can cause knee pain. Moreover, the knee often hurts even more than the hip joint itself. An X-ray is usually sufficient to confirm the diagnosis and rule out gonarthrosis.
In diseases of the spine - osteochondrosis and pinched nerve roots - the pain is very similar to coxarthrosis. However, it occurs unexpectedly, after unsuccessful movement, sharp turning of the body or lifting weights. The sensation of pain begins in the gluteal region and spreads down the back of the leg.
Radicular syndrome is characterized by severe pain when lifting a flat limb from a supine position. However, there are no difficulties in abducting the leg to the side, as in coxarthrosis. It is worth noting that osteochondrosis and osteoarthritis of the hip joint are often diagnosed at the same time, so a comprehensive examination is necessary.
Trochanteritis, or trochanteric bursitis, develops rapidly, unlike osteoarthritis, which can progress slowly over years or even decades. The pain syndrome accumulates within a week or two, and it is quite intense. The cause of trochanteritis is trauma or excessive exercise. Movement is not restricted and the leg is not shortened.
Ankylosing spondylitis and reactive arthritis may also be accompanied by symptoms that mimic coxarthrosis. Characteristic of such diseases is the appearance of pain mainly at night. The hip can hurt a lot, but when walking and moving, the pain subsides. In the morning, patients are worried about numbness, which disappears after a few hours.
Treatment of hip arthrosis
Coxarthrosis can be cured conservatively or surgically. The choice of treatment method depends on the stage and nature of the course of the pathological process. If grade 1 or 2 disease is diagnosed, it is treated with medication and physiotherapy. After relieving the acute symptoms, therapeutic exercises and massage are added. If necessary, a special diet is prescribed.
The sooner coxarthrosis is detected and treated, the better the prognosis. With the help of drugs and therapeutic measures you can significantly slow down the pathological process and improve the quality of life.
Nonsteroidal anti-inflammatory drugs (NSAIDs) are used to relieve pain and inflammation. It should be noted that anesthesia is performed in the shortest possible course, because drugs from the class of NSAIDs can adversely affect the digestive tract and slow down the regeneration processes in cartilage tissue.
With the help of chondroprotectors, it is possible to accelerate cartilage regeneration. However, these remedies are effective only in the early phase of the disease, when its hyaline cartilage is not completely destroyed. Chondroprotectors are prescribed in the form of tablets or intra-articular injections.
Vasodilators are used to improve the blood supply to the joints. Muscle relaxants are advised for muscle cramps.
In case of persistent pain syndrome, which is difficult to eliminate with tablets, injections are given in the hip joint. Corticosteroids relieve inflammation and pain well.
Drug therapy can also be supplemented with local means - ointments and gels. They do not have a pronounced effect, but they help to suppress muscle cramps and reduce pain.
Physiotherapy helps to improve blood circulation and cartilage nutrition. In coxarthrosis, procedures such as shock wave therapy (SWT), magnetotherapy, infrared laser, ultrasound and hydrogen sulfide baths have proven to be excellent.
Operation
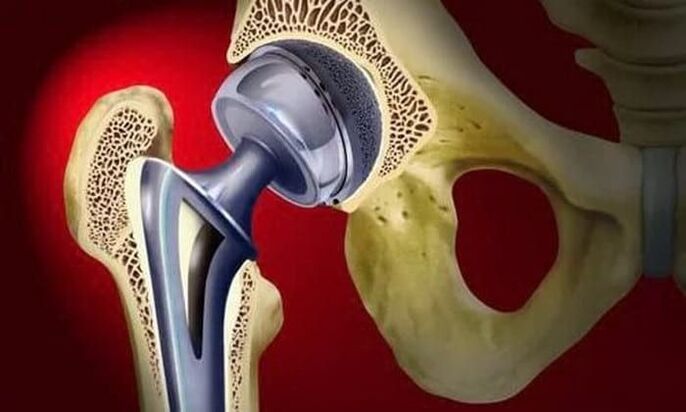
Treatment of third-degree osteoarthritis can only be surgical, as the joint is almost completely destroyed. Partial or total arthroplasty is performed to restore the function of the hip joint.
Surgical treatment is resorted to in advanced cases of osteoarthritis, when conservative therapy is powerless.
In partial prosthetics, only the femoral head is replaced with an artificial prosthesis. Total prosthetics involves the replacement of both the femoral head and the acetabulum. The operation is performed under general anesthesia, and in the vast majority of cases (about 95%) the function of the hip joint is completely restored.
During the rehabilitation period, the patient is prescribed antibiotics in order to prevent infectious complications. Threads are removed 10-12. days and exercise therapy begins. The doctor helps the patient learn to walk and properly distribute the load on the operated limb. Exercise is an important step to increase muscle strength, endurance and elasticity.
Working capacity is restored on average 2-3 months after the operation, but in the elderly this period can last up to six months. Upon completion of rehabilitation, patients can fully move, work, and even play sports. The lifespan of the prosthesis is at least 15 years. Another operation is performed to replace the worn-out prosthesis.
Effects
Without timely and adequate treatment, coxarthrosis can not only significantly worsen the quality of life, but also lead to disability and disability. Already in the second phase of arthrosis, the patient is assigned to the 3rd group of disabilities.
When shortening the affected limb by 7 cm or more, when a person moves only with the help of improvised means, another group is assigned. Group 1 disability is received by patients with grade 3 coxarthrosis, followed by complete loss of motor ability.
Indications for medical and social examination (MSC) are:
- long course of arthrosis, more than three years, with regular exacerbations. The frequency of exacerbations is at least three times every 12 months;
- undergo endoprosthetic surgery;
- severe disorders of musculoskeletal function of the extremities.
Prophylaxis
The main measures to prevent coxarthrosis are diet (if you are overweight) and regular but moderate physical activity. It is very important to avoid pelvic injuries and hypothermia.
In the presence of risk factors for arthrosis, as in all patients diagnosed with the disease, swimming is useful. Sports such as running, jumping, football and tennis are not recommended.